Greetings Everybody! I wanted to take a moment today to follow up with my original post regarding my recent research study with some of our final findings. While we have finished the study and I have completed my thesis...this information is far from completing its journey through the peer-reviewed process.
Nevertheless, here is a quick rundown/recap: We had 63 healthy and physically active college age students between the ages of 18 and 29 years that volunteered for this study. All participants were randomly allocated into one of three groups by an online random group allocation generator. We hoped to have more subjects in this study but I ran out of time to recruit more and I needed to cut my losses if I wanted to finish the study and graduate on time. One group received the foot-toe orthosis (Correct Toes - FTO ) and the control shoe (Lems Primal 2 - SO), one group received the control shoe only, and one group was a true control (CON) that received neither intervention. The following table displays our group demographics...ideally I wish we could have made the groups perfectly even and had more subjects overall.
Just to review, we used the Lower Quarter Y-Balance Test (YBT-LQ) as our measure of dynamic balance. I’m not going to go over all of the procedures and what not again because you can find all of that information in the above link from the original post. So why don’t we just get down to the fun part...The Findings.
There is a lot of numbers in that table...and it isn’t very pretty. Nevertheless, it does tell us some important information. After adjusting for baseline scores (ANCOVA) there were significant differences between the post-intervention scores on the YBT-LQ. This means that there was a statistically significant difference (p=.001) between the groups at follow-up testing. Also, these YBT-LQ scores are the composite scores. That means they are the maximum reach directions for each reach direction(anterior, posteromedial, and posterolateral), and then normalized for apparent leg length.
Pairwise comparisons revealed that the FTO group was significantly different (p=.001) from the CON group. There was also a significant difference (p=.034) between the SO and CON groups. Additionally, the FTO group was significantly different (p=.007) than the SO group. The FTO group had a strong effect size of .70 while the SO group had a moderate effect size of .45. Phew, that paragraph sounded a lot like a journal article...So lets use a pretty graph to highlight this information even further and it is much easier on the eyes.
So what does this all mean? The purpose of our study was to see if the foot-toe orthosis had any effect on dynamic stability. Our results were the first to show that this type of orthosis could be used to increase dynamic balance with 4 weeks of use in a healthy, young-adult population. These results were similar to other interventions to increase dynamic balance/postural stability using mediums such as textured surfaces, insoles and traditional orthoses. However, due to the difference in metrics and intervention choice...direct comparison isn't really feasible.
There are several theories abound for why such interventions may be efficacious such as increase afferent input to the feet/toes and the potential for passively increasing the base of support. However, it was beyond the scope and aim of this study to determine why they work and unfortunately we didn’t enough measures to control well enough to check on some of these theories.
We do know that when wearing the foot-toe orthosis the base of support is certainly increased, yet pre and post data collection was done without the use of the foot-toe orthosis. This means the increased dynamic balance was not reliant upon the foot-toe orthosis. Additionally, the control shoe only group saw an increase in dynamic balance as well.
This could be attributed that the control shoe was technically advertised as a“minimalist” shoe by manufacturer and despite a lack of universal definition for a minimalist shoe...I would have to agree that this shoe was minimally cushioned, zero drop (ramp from heel to forefoot), offered no support to the foot beyond grip, and had a wider toe box than most traditional footwear. This design could potentially work to increase dynamic balance through increasing the base of support and allowing better afferent input.
In conclusion, our results suggest that the use of the foot-toe orthosis and the control shoe may increase dynamic balance in a healthy and college-aged population. The moderate to strong effect sizes associated with our results are promising; However, it is imperative that future research be conducted to investigate the effects in differing populations such as the elderly, the injured, and people with neuropathic conditions such as diabetes. It must also be investigated on whether these findings have any impact on injury risk and to determine what the long-term effects of use. This information could help researchers or clinicians investigate potential treatment or prophylactic approaches.
Today's post is kind of half personal story/half conjecture/half observation(wait, that doesn't add up!). To begin, I have now been wearing a minimalist/zero drop type shoe everyday for both casual use and exercise/running. The only time I wear a shoe that is not completely flat is when I wear my dress shoes with my suit for basketball games.
One of my current favorites
I am a huge proponent of wearing zero drop shoes with a wide toe box and the absence of a "toe spring". I feel this shoe design interferes the least with proprioception, normal foot mechanics, and proper tissue length. Think of non-zero drop shoes as being like a mini-high heel.
I have put together a video compilation of some of my favorite mobility and strengthening exercises for the foot. The target of most of these will be for the intrinsic soft tissues of the feet but you can't fully target just one area or muscle of the body with an exercise. I didn't think of all of these ideas and I tried to give credit to those that I learned them from where I could!
These would be good for anyone with a history of ankle, lower leg or foot injuries. It doesn't matter if you wear Hoka One Ones or nothing on your feet because all of us should have strong and mobile feet. Your feet do a ton of work for you and are your main contact point with the ground. Take care of them!
Hey everyone, I was about to go for a run today and I thought of the idea of highlighting some of repeated-end range exercises that I have mentioned in some of my recent posts. Today I will show you two of them that I do try to do before every one of my runs. I learned these from Dr. Erson of TheManualTherapist.com so I can't take credit for thinking of them! I must say that incorporating these two exercises has helped me resolve any lingering heel stiffness/pain that I previously had.
It is very easy to find out if these will do anything for you by giving them a try and checking your mobility to see if benefit from them. If you do, great! If not, you might want to try some soft tissue to assist you reach your true end range or maybe just find something that does work for you!
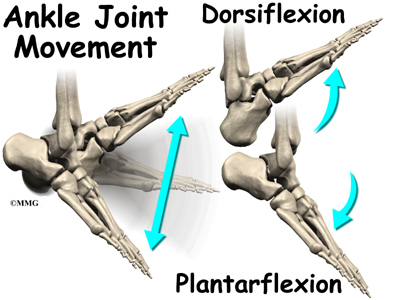
Dorsiflexion. This important motion occurs at the ankle and is seen when the dorsal(top) aspect of the foot and the anterior(front) aspect of the tibia(shin) move closer together. This motion is seen with and is necessary for proper execution of many basic human movements including squatting, running, walking, jumping and more. This motion is a vital part of most functional movements and proper function up and down the entire kinetic chain. Even minor tasks such as sitting and standing from a chair or walking up and down stairs requires adequate dorsiflexion of the ankle.
There are many issues related to inadequate dorsiflexion including many lower extremity injuries and and foot deformities. Evidence exists that problems here can be related to falls in the elderly, patellar tendinopathy, ACL injuries, lower extremity kinematic changes, and patellofemoral pain syndrome to name a few. This motion could be limited by several different problems such as soft tissue mobility(muscles and fascia), bony abnormalities, joint capsule restrictions(belongs with soft tissue mobility), and impingement of these structures.
The human foot and ankle are masterpieces of complexity and natural engineering.
When a person is deficient in dorsiflexion they are not automatically limited in the aforementioned movements(besides dorsiflexion, duh) or tasks such as a squat. The human body is great at incorporating compensatory movements to allow a continuance of motion to increase our ability to survive but at the cost of our ability to thrive.
For example, lets say I have a patient named Jim Shorts who comes to me with complaints of knee and low back pain as well as a history of chronic plantar fasciosis. Jim loves going jogging, playing basketball, and working in the garden with his wife.
These are very common symptoms and could be caused by a variety of issues but for the sake of this post lets discuss how they could be related to dorsiflexion of the ankle. Before we even begin to evaluate Mr. Shorts lets think about how dorsiflexion might be needed during each these activities.
Running
The ankle plantar flexors(think calf muscles) and plantar fascia may be eccentrically (resistively stretched) loaded at initial foot strike depending on landing type (heel strike vs mid-forefoot landings).
Initial Contact
As the gait cycle changes from initial contact to mid-stance, the ankle moves into a more dorsiflexed position. At this moment, vertical ground reaction forces are at their highest(Active Peak on the graph below) and loading of the achilles tendon is reaching its maximum peak. To allow proper dispersal of these forces and to allow some of this energy to be stored and then reused the achilles must act as a spring. Dr. Mark Cuccuzzella has made a video that highlights these principles of running mechanics and he does a much better job of visually and audibly explaining it than I can in writing.
Steve Magness, writer of the blog Science of Running, and Head Cross Country coach at the University of Houston wrote a great post on the most vital components of running here as well.
Midstance
The ankle plantar flexors are now on maximum stretch(maximum dorsiflexion) and are maximally loaded now must assist the posterior chain(gluteus muscles and hamstrings) to propel the body forward and slightly upward(propulsion phase & toe-off).
These components involving the ankle and its ability to dorsiflex are vital to running and any sports that involve running. If motion is impaired we should not expect to be efficient or safe from injury. Would you expect a car to have maximum performance or to be safe from harm if you had improperly sized or damaged shocks?
I like the analogy of the ankle plantar flexors to be a group of rubber bands. If you have soft tissue problems then these rubber bands may be tied full of knots or could be thought of as dried out and having lost their snap. If you have bony or joint capsule restrictions then you may not have the ability properly stretch out a healthy rubber band to allow maximum performance or perhaps this inability caused a degradation in the health of the rubber band itself. Double Jeopardy.
Basketball & Gardening
Requires the ability to run(discussed previously)
Requires the ability to jump
You need to be able to shoot a jump-shot, lay-up, dunk or to go up for a rebound.
Requires the ability to land after jumping
You need to safely come down after jumping and be able to dissipate the forces from impacting the ground.
The above can be summarized by the ability to squat. (*Only the squat applies to gardening, unless you are into some extreme gardening stuff that i've never heard of before.)
You also need to be able to properly squat to get into sport-specific positions of basketball such as a defensive stance and you don't want to bend at the waist to work in your garden(some people still will).
Looking at Mr. Shorts
So we begin to evaluate Mr. Shorts and we have him perform some functional movements to evaluate his movement behavior. For example, we ask Jim Shorts to do a deep squat like he would while gardening and we notice that his heels can not touch the ground and he excessively flexes his trunk forward to allow his arms to work at ground level.
Next, I have Jim show me his defensive basketball stance. We immediately notice that his knees extend past his toes and that he has that same forwardly flexed trunk position as before. He also complains that this position immediately exacerbates the pain in his knees and low back.
At this point I decide to try something. I take either a heel lift and place it into Jim's shoes or place his heels onto a 2in. board and have him repeat his deep squat. This time Mr. Shorts is able to squat down with his heels flush to the ground (or board) and his back appears to be parallel with his shins from a side view. The only difference here is that we eliminated the demand for proper dorsiflexion. Technically, this might not be the only reason for his limitations but I wanted to show how improper dorsiflexion could change a functional movement.
This example shows us how problems with movement at the ankle can increase forces and perhaps damage tissues further up the kinetic chain. The next step for us would be to decipher what type of dorsiflexion restriction Jim Shorts actually has but that post is for another day so lets move on to figuring out how to evaluate your own ankle dorsiflexion.
Self Evaluation
Lets discuss how you can evaluate your own ability to dorsiflexion at home. Here are a few links to some of my favorite techniques and how-tos for evaluating ankle mobility.
This first link is credited to Mike Reinold's blog and is an all-encompassing post that is very concise and does a great job of saying everything that I am trying to say with this post. He even has many great videos for working on improving your own mobility.
This link is to a blog post by Jay Dicharry, MPT, CSCS...Author of the book, Anatomy for Runners. Jay is probably one of the premier clinicians and researchers out there today when it comes to running mechanics, research and injuries. This post discusses more than just ankle dorsiflexion and is definitely recommended.
This next link is actually to a video made by Jay Dicharry. This video will show you a quick and easy list of self-evaluation techniques and fixes for somebody looking to transition to minimal running shoes. However, I feel that these are vital to athletes and runners regardless if they are barefoot or wearing Hoka one-ones.
How much dorsiflexion do you actually need? Jay Dicharry recommends at least 25 degrees of dorsiflexion at the ankle and 30 degrees of dorsiflexion of the big toe(measured at 5 degrees of ankle dorsiflexion). Mike Reinold and the minds of the Functional Movement System, such as Gray Cook sponsor the idea of the knee reaching about 5 inches past the toes while in a half kneeling stance. One study found that athletes with less than 36.5 degrees of dorsiflexion had an..."18.5 to 29.4% risk of developing patellar tendinopathy compared to a 1.8 to 2.1% risk for athletes with dorsiflexion greater than 36.5 degrees." I believe most of these values to be too similar to chose one set of thought over the other and suggest them as mere guidelines and not cut points.
How do I fix this?
I had originally planned on writing an entire section on my favorite joint mobilization, static stretching, and soft tissue mobilization techniques but the links I provided in the self-evaluation section have some great techniques included with them already. I feel like I can not top those techniques and I highly recommend them. However, I do want to summarize some thoughts about trying to increase dorsiflexion.
I believe that a vast majority of us living in 1st world countries that grew up with or have been wearing shoes for decades with an elevated heel have limitations in ankle dorsiflexion. There are exceptions to this but I have provided you with information to check for yourself.
I admit that going barefoot or utilizing a more minimal shoe during training may not be feasible for everyone. However, I do feel that incorporating and wearing a shoe with less heel-to-toe drop or less of an elevated heel during everyday activities such as at work, around the house or out on the town can be very beneficial for restoring proper ankle dorsiflexion. What you wear on your feet 90% of the time probably has a more profound effect on your tissues than the shoes you wear 5-10% of time you spend training each week.
When it comes to increasing the actual mobility with manual work I believe a multi-faceted approach is best. A combination of joint mobilizations, static stretching(post exercise), foam rolling, etc is probably going to be more effective for you unless you or a manual therapist has determined that only one specific issue is limiting you. It would not be uncommon for several of these issues to be a limiting factor for a person.
Do not ignore above and below, tibial internal & external rotation as well as plantar fascia mobility influence movement at the ankle as well.
DO NOT try to treat the symptom by eliminating the need for proper dorsiflexion. Utilization of heel lifts, immobilization, restrictive tape jobs, new shoes and etc. are only treating your symptoms. These MAY be appropriate for short-term relief but they do NOT fix your problem. If you try to take the easy way out and try to eliminate this motion then you are setting yourself up for a different set of problems up and down your entire kinetic chain.
In conclusion, this is going to be an issue with a majority of people. This problem exists in both the physically active and inactive populations. Only the minority of people that I've tested have had adequate ankle dorsiflexion. I would love to see how this compares with a third world country where people have not had the "luxury" of wearing shoes with elevated heels since birth. I bet you can find plenty of pictures in a national geographic magazine where the indigenous tribespeople have perfect squat form and can hold it comfortably with ease.
Updates
Here are a few related videos that I have made that should be of value to this topic as well! Enjoy!
Disclaimer: Please note that some of the links on this blog are affiliate links and I will earn a commission if you purchase through those links. I have used all of these products listed and recommend them because they are helpful and are products from companies that I trust, not because of the commissions that I may earn from you using these products.
Caution
All content on this blog is meant as instructional and educational. The author and guest authors of this blog are not responsible for any harm or injury that may result. Always consult a physician or another proper medical professional for medical advice.


 There is a lot of numbers in that table...and it isn’t very pretty. Nevertheless, it does tell us some important information. After adjusting for baseline scores (ANCOVA) there were significant differences between the post-intervention scores on the YBT-LQ. This means that there was a statistically significant difference (p=.001) between the groups at follow-up testing. Also, these YBT-LQ scores are the composite scores. That means they are the maximum reach directions for each reach direction(anterior, posteromedial, and posterolateral), and then normalized for apparent leg length.
There is a lot of numbers in that table...and it isn’t very pretty. Nevertheless, it does tell us some important information. After adjusting for baseline scores (ANCOVA) there were significant differences between the post-intervention scores on the YBT-LQ. This means that there was a statistically significant difference (p=.001) between the groups at follow-up testing. Also, these YBT-LQ scores are the composite scores. That means they are the maximum reach directions for each reach direction(anterior, posteromedial, and posterolateral), and then normalized for apparent leg length.




.JPG)








.gif)
.JPG)


