For my second and final year of graduate school I will be featured as a semi-regular guest blogger at ATC Hacks. The series will be called "Grad Life" and as you might guess it will be about my time as a graduate student and graduate assistant athletic trainer.
I will be discussing things like advice for prospective graduate students, reflections on my own experiences, and anecdotes related to my own trials and tribulations. Here is a link to my first post! It isn't very long or informative, it is just more of an introductory post! This is the same website that featured me on their "In The ATR" series and you can find that post here if you haven't checked it out yet.
My next post will be my 50th blog post which I am considering a mini milestone, so I hope that I can make it something interesting for you all! To also go along with that piece of news is the fact that you can now type in EatRunRehab.com and it will redirect you to my site. No more worries about the long URL or spelling rehabilitate correctly! ;)
The weekend is finally here and that means you might have some more free time on your hands. If that is the case then here are some recent and interesting reads for you all. They are split up by genre! ;)
I am not sure if the title of this post makes any sense but what I am trying to say is that I am itching to get back into the clinic. All of my athletes(patients) are on summer break and I won't be dealing with any athletes for another two weeks or so. I love being an athletic trainer and I have been reading/watching/learning a lot this summer that I want to use to advance my skills as a clinician.
With no athletes to fix I have resorted to offering a helping hand to others outside of my athletic training world. I work as a barista for a part-time summer job to help foot some of my bills and fortunately for me over the past week this job has been a source for me to help some people with musculoskeletal issues.
I have put together a video compilation of some of my favorite mobility and strengthening exercises for the foot. The target of most of these will be for the intrinsic soft tissues of the feet but you can't fully target just one area or muscle of the body with an exercise. I didn't think of all of these ideas and I tried to give credit to those that I learned them from where I could!
These would be good for anyone with a history of ankle, lower leg or foot injuries. It doesn't matter if you wear Hoka One Ones or nothing on your feet because all of us should have strong and mobile feet. Your feet do a ton of work for you and are your main contact point with the ground. Take care of them!
Here comes another rant or a pet peeve that I have related to recent warm weather and people exercising in it. Just like this photo displays I hate that people think safely exercising in warm weather is all about preventing dehydration, and drinking copious amounts of fluids. Some athletes and coaches think that they can work vigorously and non-stop in extreme conditions as long as there is an adequate water supply. It doesn't matter how much you drink, it won't prevent your core body temperature from rising. The real danger is exercising in a way that allows the core temperature to reach unsafe levels where heat stroke can occur.
Concussions are still a hot topic and will continue to be for the foreseeable future. The media loves to discuss them, coaches loathe them, parents fear them, and the research is still within its infancy. It isn't time for anyone to jump to conclusions or panic but it is definitely a good time to stay informed and properly educated on the topic. This blog post came as a result of the latest edition of the Journal of Athletic Training, which had several concussion related articles. To begin the issue there was a special editorial written by concussion research expert, Kevin Guskiewicz, PhD, ATC, FNATA, FACSM. He is also the chair of the Department of Exercise and Sport Science at the
University of North Carolina at Chapel Hill. Dr. Guskiewicz recommends that sports medicine professionals stay informed on upcoming concussion research to be published within the next 6 months. This includes the ‘‘Consensus statement on concussion in sport: the 4th International Conference on
Concussion in Sport, Zurich, November 2012’’ that was published in this edition of the Journal of Athletic Training and originally published in the British Journal of Sports Medicine in March, 2013. He advises that these documents "will
define the standard of care for athletic trainers and team
physicians for at least the next 4 to 5 years. These
documents are very well prepared and will make significant
contributions to the sports medicine community." He also had these three major closing points:
Read these documents,
Develop and implement a sound concussion-management program and policy
Check the boxes each time you manage a patient with a concussion.
Dr. Guskiewicz had one last closing piece of advice that is very important for concussion management but is applicable to everything we do as clinicians and arguable important for any person to learn. I know football season for me is fast approaching so I know I need to make sure I get caught up on my concussion literature. I will leave you with his advice in quotes and a link to the latest journal issue!
"But just as important, be sure you go the extra mile to educate yourself and your athletes and to ensure that both
you and your athletes are protected. "
Therapeutic modalities had an entire course devoted to it in my educational curriculum and there is more and more research being done on the topic. There is plenty to learn about the theory and application of each individual type of modality from ultrasound to electrical stimulation and plain old ice.
I definitely learned a lot and the use of modalities has been definitely beneficial for me as a clinician, especially for acute injuries. However, I have found myself and others at fault for relying upon modalities too much. There are too many clinicians relying upon the "powers" of modalities instead of using the power of movement and rehabilitative exercises. I'm not saying that they don't have their place because they definitely do but they often are too heavily relied upon.
Eat Yesterday, Chris Kresser announced that his book now available for pre-sale. If you haven't checked out his website, ChrisKresser.com, then you are missing out on some quality articles related to health and nutrition. His book will be titled Your Personal Paleo Code and will be released on Christmas Eve. Run Coach Caleb of Team BonkProof wrote a short article about dealing with the heat and humidity during these dog days of summer. I like this article and feel his advice is on target with the science related to how we should go about hydrating and exercising in the heat. Great training tips, Coach! Dr. Nick Campitelli, DPM is featuring a story on his blog of a runner that has overcome chronic knee pain by successfully and safely transitioning to minimalist running. This find technically belongs in both the Run and Rehabilitate section...Love it when that happens ;). Rehabilitate Erson Religioso of TheManualTherapist posted a blog and video about using his EDGE Mobility bands as an alternative approach to using a mobilization belt for increasing Hip Internal Rotation. I haven't personally attempted this because I don't have any EDGE bands yet, but this seems much more time and user friendly than the bulky mobilization belts. I don't own any of those either actually... Here is an interesting editorial by Richard Demont, PhD, CAT(C), ATC in the latest edition of Athletic Training & Sports Health Care about athletic trainers needing to promote our profession through quality research initiatives. This is an article that rings true for me considering I am working on my first research study for my master's thesis and I want it to be a quality and credible piece of work in the end.
I was recently asked by the guys over at ATCHacks if I was willing to answer some questions for their "In The ATR" series. I have been following @ATCHacks on twitter for awhile now and I love what they have been doing, what they are about and how they are doing good things for the profession of Athletic Training. Their "In The ATR" series features athletic trainers and asks them questions about their history, methods, tips and med-kits. I was not only honored to have them ask me to be part of In The ATR, but they have also asked me on to regularly guest blog for them about my experiences as a graduate assistant athletic trainer. This next year is going to be an exciting and fast paced time for me! Head on over ATC Hacks to see their feature on me and don't be afraid to register at their site to get full access to their information for free. They have some insightful articles for athletic trainers and aspiring athletic training students.
I am quickly reaching my one year anniversary since finishing my undergraduate education and becoming a certified athletic trainer. A lot has happened since then including starting work on my master's degree, my master's thesis and working with many different athletes and teams via my graduate assistant position. I have learned a lot and it would be impossible to list everything but I figured it would be a good idea to reflect back on a few major themes.
Somehow, someway during my initial years of schooling I
developed this idea that the profession of athletic training needed to compete
heavily with other professions. I used to think that I needed to boycott the
teachings of other professions like physical therapists, strength and
conditioning specialists and person trainers. I also had an urge to compete against others within my own
profession and try to be most intelligent or most competent clinician/academic. Finishing school and starting my professional career has definitely changed my thought processes.
While some level of competitiveness is necessary in a world
where multiple professions compete for patients or clients from the same pool
of people due to similar skill sets. However, I have begun to realize that this
previous thought process hurt three groups of people. Thinking and behaving the
way I did disadvantaged myself (the clinician), potential patients, and the
different professions.
Recently, I have worked to open myself up to the ideas of
others and other professions. Just think, where would human intelligence even
be now without the collective body of knowledge that is shared between
individuals? We might be able to think the same but the accumulation of
knowledge that is passed around and down through time is what makes it special.
Hey everyone, I was about to go for a run today and I thought of the idea of highlighting some of repeated-end range exercises that I have mentioned in some of my recent posts. Today I will show you two of them that I do try to do before every one of my runs. I learned these from Dr. Erson of TheManualTherapist.com so I can't take credit for thinking of them! I must say that incorporating these two exercises has helped me resolve any lingering heel stiffness/pain that I previously had.
It is very easy to find out if these will do anything for you by giving them a try and checking your mobility to see if benefit from them. If you do, great! If not, you might want to try some soft tissue to assist you reach your true end range or maybe just find something that does work for you!
I have been following Dr. Erson Religioso's blog, The Manual Therapist, for quite some time now. I also recently subscribed to his OMPT Channel section where I have learned quite a few evaluation and treatment techniques to add to my arsenal. Dr. E has training in a plethora of different schools of thought and one of them is the Mechanical Diagnosis and Therapy or MDT for short. Part of his MDT skill-set is a various amount of techniques that he refers to as "resets". He often uses them as part of his evaluation, treatment and home exercise programs. I hope I am saying all of this accurately, at least. Here is a couple videos of Dr. Erson Religioso III, DPT, FAAOMPT explaining the what, why and how related to these resets.
This is Dr. E's video highlighting the his favorite resets, and why they work.
An updated but longer video for Dr. E's favorite resets.
The Toe Pain:
I am currently pursuing a post-professional graduate degree so that means I am still a student (will be one for life) and that I still have finals. A couple Monday’s ago I was sitting around with a few of my classmates while waiting to take a final practical exam. One classmate mentioned that she had a very painful big toe on her right foot. She had been suffering this pain for a day or two since walking around Chicago the entire weekend while wearing ill-fitting footwear. She had only had the pain on one side without any direct MOI besides gradual onset related to the shoes and walking. She had pain with great toe extension when toeing-off in her gait cycle.
Dr. E’s videos had been on my mind and I was curious if his resets would really work because they were a foreign concept related to anything I had been taught. I had the idea of doing repeated-end range flexion of the great toe for about 20 repetitions and I asked her if she minded trying out the experiment. She obliged and we went to town with the repeated “resets”.
After I finished with the 20 or so repeats I asked her to stand up and walk around. Alas, she had no pain and no other complaints appeared. I told her that there was a chance that this would be a transient effect and that she may need to repeat this exercise about 10 times every hour. However, her pain never returned that day and hasn’t to date. I believe a week later when I inquired about her toe she mentioned that my “voodoo” had fixed the issue for good. While I don’t think I was doing any magic or voodoo I do think this highlights some merit to these resets on an n=1 level. Half of evidence-based practice is clinical experience and so far my “clinical” experience has been great; although I do wish I had some more extensive training or knowledge about MDT. I was impressed enough with these results that I tried using the repeated ankle plantar flexion reset for my girlfriend’s aunt who has had years of constant heel pain. This was just an offhand encounter at Mother’s Day brunch but it immediately took her symptoms from a wince-inducing 8/10 to a 4/10. I gave her instructions to continue these as a self-empowering home exercise and I hope she sticks to them. I really want to see how she progresses.
Conclusion:
My conclusion about these resets so far is that I like them but I don’t see them as a replacement to my current clinical skill set. I see them as being another tool and a great way to put responsibility into the hands of the patient. I understand the theory and concept as explained by Dr. Religioso. However, I definitely feel and want to learn more about this stuff before it starts to become a mainstay of my clinical practice.
Today I wanted to showcase a mini-case study of an athlete
that I consulted with recently. This was a 22 year old female collegiate track
and field athlete. This patient was a mid-distance runner that specialized in
the 800m event.
http://trialx.com/g/Calf_Pain-1.jpg
The athlete complained of chronic pain at the
musculotendinous junction of the Achilles tendon that had been recurrent at the
beginning of track season the previous two years. The athlete had a previous
history of turf-toe like symptoms in the ipsilateral great toe.
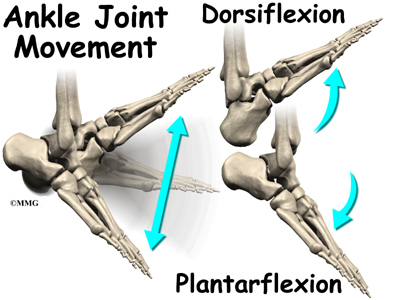
Dorsiflexion. This important motion occurs at the ankle and is seen when the dorsal(top) aspect of the foot and the anterior(front) aspect of the tibia(shin) move closer together. This motion is seen with and is necessary for proper execution of many basic human movements including squatting, running, walking, jumping and more. This motion is a vital part of most functional movements and proper function up and down the entire kinetic chain. Even minor tasks such as sitting and standing from a chair or walking up and down stairs requires adequate dorsiflexion of the ankle.
There are many issues related to inadequate dorsiflexion including many lower extremity injuries and and foot deformities. Evidence exists that problems here can be related to falls in the elderly, patellar tendinopathy, ACL injuries, lower extremity kinematic changes, and patellofemoral pain syndrome to name a few. This motion could be limited by several different problems such as soft tissue mobility(muscles and fascia), bony abnormalities, joint capsule restrictions(belongs with soft tissue mobility), and impingement of these structures.
The human foot and ankle are masterpieces of complexity and natural engineering.
When a person is deficient in dorsiflexion they are not automatically limited in the aforementioned movements(besides dorsiflexion, duh) or tasks such as a squat. The human body is great at incorporating compensatory movements to allow a continuance of motion to increase our ability to survive but at the cost of our ability to thrive.
For example, lets say I have a patient named Jim Shorts who comes to me with complaints of knee and low back pain as well as a history of chronic plantar fasciosis. Jim loves going jogging, playing basketball, and working in the garden with his wife.
These are very common symptoms and could be caused by a variety of issues but for the sake of this post lets discuss how they could be related to dorsiflexion of the ankle. Before we even begin to evaluate Mr. Shorts lets think about how dorsiflexion might be needed during each these activities.
Running
The ankle plantar flexors(think calf muscles) and plantar fascia may be eccentrically (resistively stretched) loaded at initial foot strike depending on landing type (heel strike vs mid-forefoot landings).
Initial Contact
As the gait cycle changes from initial contact to mid-stance, the ankle moves into a more dorsiflexed position. At this moment, vertical ground reaction forces are at their highest(Active Peak on the graph below) and loading of the achilles tendon is reaching its maximum peak. To allow proper dispersal of these forces and to allow some of this energy to be stored and then reused the achilles must act as a spring. Dr. Mark Cuccuzzella has made a video that highlights these principles of running mechanics and he does a much better job of visually and audibly explaining it than I can in writing.
Steve Magness, writer of the blog Science of Running, and Head Cross Country coach at the University of Houston wrote a great post on the most vital components of running here as well.
Midstance
The ankle plantar flexors are now on maximum stretch(maximum dorsiflexion) and are maximally loaded now must assist the posterior chain(gluteus muscles and hamstrings) to propel the body forward and slightly upward(propulsion phase & toe-off).
These components involving the ankle and its ability to dorsiflex are vital to running and any sports that involve running. If motion is impaired we should not expect to be efficient or safe from injury. Would you expect a car to have maximum performance or to be safe from harm if you had improperly sized or damaged shocks?
I like the analogy of the ankle plantar flexors to be a group of rubber bands. If you have soft tissue problems then these rubber bands may be tied full of knots or could be thought of as dried out and having lost their snap. If you have bony or joint capsule restrictions then you may not have the ability properly stretch out a healthy rubber band to allow maximum performance or perhaps this inability caused a degradation in the health of the rubber band itself. Double Jeopardy.
Basketball & Gardening
Requires the ability to run(discussed previously)
Requires the ability to jump
You need to be able to shoot a jump-shot, lay-up, dunk or to go up for a rebound.
Requires the ability to land after jumping
You need to safely come down after jumping and be able to dissipate the forces from impacting the ground.
The above can be summarized by the ability to squat. (*Only the squat applies to gardening, unless you are into some extreme gardening stuff that i've never heard of before.)
You also need to be able to properly squat to get into sport-specific positions of basketball such as a defensive stance and you don't want to bend at the waist to work in your garden(some people still will).
Looking at Mr. Shorts
So we begin to evaluate Mr. Shorts and we have him perform some functional movements to evaluate his movement behavior. For example, we ask Jim Shorts to do a deep squat like he would while gardening and we notice that his heels can not touch the ground and he excessively flexes his trunk forward to allow his arms to work at ground level.
Next, I have Jim show me his defensive basketball stance. We immediately notice that his knees extend past his toes and that he has that same forwardly flexed trunk position as before. He also complains that this position immediately exacerbates the pain in his knees and low back.
At this point I decide to try something. I take either a heel lift and place it into Jim's shoes or place his heels onto a 2in. board and have him repeat his deep squat. This time Mr. Shorts is able to squat down with his heels flush to the ground (or board) and his back appears to be parallel with his shins from a side view. The only difference here is that we eliminated the demand for proper dorsiflexion. Technically, this might not be the only reason for his limitations but I wanted to show how improper dorsiflexion could change a functional movement.
This example shows us how problems with movement at the ankle can increase forces and perhaps damage tissues further up the kinetic chain. The next step for us would be to decipher what type of dorsiflexion restriction Jim Shorts actually has but that post is for another day so lets move on to figuring out how to evaluate your own ankle dorsiflexion.
Self Evaluation
Lets discuss how you can evaluate your own ability to dorsiflexion at home. Here are a few links to some of my favorite techniques and how-tos for evaluating ankle mobility.
This first link is credited to Mike Reinold's blog and is an all-encompassing post that is very concise and does a great job of saying everything that I am trying to say with this post. He even has many great videos for working on improving your own mobility.
This link is to a blog post by Jay Dicharry, MPT, CSCS...Author of the book, Anatomy for Runners. Jay is probably one of the premier clinicians and researchers out there today when it comes to running mechanics, research and injuries. This post discusses more than just ankle dorsiflexion and is definitely recommended.
This next link is actually to a video made by Jay Dicharry. This video will show you a quick and easy list of self-evaluation techniques and fixes for somebody looking to transition to minimal running shoes. However, I feel that these are vital to athletes and runners regardless if they are barefoot or wearing Hoka one-ones.
How much dorsiflexion do you actually need? Jay Dicharry recommends at least 25 degrees of dorsiflexion at the ankle and 30 degrees of dorsiflexion of the big toe(measured at 5 degrees of ankle dorsiflexion). Mike Reinold and the minds of the Functional Movement System, such as Gray Cook sponsor the idea of the knee reaching about 5 inches past the toes while in a half kneeling stance. One study found that athletes with less than 36.5 degrees of dorsiflexion had an..."18.5 to 29.4% risk of developing patellar tendinopathy compared to a 1.8 to 2.1% risk for athletes with dorsiflexion greater than 36.5 degrees." I believe most of these values to be too similar to chose one set of thought over the other and suggest them as mere guidelines and not cut points.
How do I fix this?
I had originally planned on writing an entire section on my favorite joint mobilization, static stretching, and soft tissue mobilization techniques but the links I provided in the self-evaluation section have some great techniques included with them already. I feel like I can not top those techniques and I highly recommend them. However, I do want to summarize some thoughts about trying to increase dorsiflexion.
I believe that a vast majority of us living in 1st world countries that grew up with or have been wearing shoes for decades with an elevated heel have limitations in ankle dorsiflexion. There are exceptions to this but I have provided you with information to check for yourself.
I admit that going barefoot or utilizing a more minimal shoe during training may not be feasible for everyone. However, I do feel that incorporating and wearing a shoe with less heel-to-toe drop or less of an elevated heel during everyday activities such as at work, around the house or out on the town can be very beneficial for restoring proper ankle dorsiflexion. What you wear on your feet 90% of the time probably has a more profound effect on your tissues than the shoes you wear 5-10% of time you spend training each week.
When it comes to increasing the actual mobility with manual work I believe a multi-faceted approach is best. A combination of joint mobilizations, static stretching(post exercise), foam rolling, etc is probably going to be more effective for you unless you or a manual therapist has determined that only one specific issue is limiting you. It would not be uncommon for several of these issues to be a limiting factor for a person.
Do not ignore above and below, tibial internal & external rotation as well as plantar fascia mobility influence movement at the ankle as well.
DO NOT try to treat the symptom by eliminating the need for proper dorsiflexion. Utilization of heel lifts, immobilization, restrictive tape jobs, new shoes and etc. are only treating your symptoms. These MAY be appropriate for short-term relief but they do NOT fix your problem. If you try to take the easy way out and try to eliminate this motion then you are setting yourself up for a different set of problems up and down your entire kinetic chain.
In conclusion, this is going to be an issue with a majority of people. This problem exists in both the physically active and inactive populations. Only the minority of people that I've tested have had adequate ankle dorsiflexion. I would love to see how this compares with a third world country where people have not had the "luxury" of wearing shoes with elevated heels since birth. I bet you can find plenty of pictures in a national geographic magazine where the indigenous tribespeople have perfect squat form and can hold it comfortably with ease.
Updates
Here are a few related videos that I have made that should be of value to this topic as well! Enjoy!
Howdy potential future readers. I am not sure if I will ever get any future readers but hello if I somehow do garner your attention. I am starting my first blog, this blog, because I would like to create a source or forum where I can communicate ideas with others who may or may not have similar ideas with myself. This type of atmosphere can help me learn from others, help others or debate with others.
The fact that nobody agrees on anything is great. It is a good thing in the world of science and it keeps the regular world from becoming too boring. I would like to write about topics that interest me and as a 23 year old graduate student and Certified Athletic Trainer (not trainer) I have interests in diet, running, health, science, cycling and health care. Some may feel like the future posts will be too far ranging at times but I see all of these topics as inter-related and integrated with each other.
I hope to share personal stories, stories of others, related news and articles of research related to the aforementioned topics and more. I am not promising myself or anyone that I am an English laureate. I can't even promise myself that my writing can rival the average 5th grader's writing but I will attempt to create legible posts for your sake.
My first real post will be based upon the topic of the never pleasant runner's trots and its relationship with diet. This preview to my first topic might repel some potential readers and it may catch the attention of others. Just like runner's trots, it is probably a risk that I shouldn't take.
Below is a couple of pictures of myself to help give voice to my writing.
Disclaimer: Please note that some of the links on this blog are affiliate links and I will earn a commission if you purchase through those links. I have used all of these products listed and recommend them because they are helpful and are products from companies that I trust, not because of the commissions that I may earn from you using these products.
Caution
All content on this blog is meant as instructional and educational. The author and guest authors of this blog are not responsible for any harm or injury that may result. Always consult a physician or another proper medical professional for medical advice.









.JPG)










.gif)
.JPG)


