
Howdy Readers! After yesterday's post ice seems to be a hot topic. I may have misled some of you yesterday with my thoughts on ice. Like many things in healthcare, science, and research the answers to questions are often shades of grey...not black and white like many would prefer. Therefore, today I wanted to share with all of you a guest post that I wrote for another website regarding a study that showcased a time when icing is warranted and was found to be very beneficial. This isn't the first article that shows evidence for this idea but it is the most recently published.
Additionally, I wanted to hammer home the idea that ice can still be used to modulate pain...if a 14 year old high school athlete suffers a severe ankle sprain for the first time and is in a lot of pain it would be unethical and unreasonable to deny him a bag of "ice" because research shows that it may not change blood flow. I can still help to modulate his pain without the use of narcotics or NSAIDs (a whole different bag of worms).
Nevertheless, pain should still be viewed as a perception and as something that can alter movement/motor control. We do not want to associate pain purely with structural damage because we know that is not the case based off the latest pain science. What I am against however is clinicians that ice to "treat" or "fix" injuries instead of using sound clinical reasoning, causative biomechanics, and taking pain science into consideration. We need to question the mechanism of why we are choosing a certain treatment, exercise, or modality. Enough with the ranting, here is my article!
 |
| Source: http://pds.exblog.jp/pds/1/201404/11/09/b0112009_5555964.png |
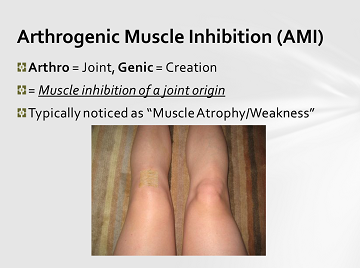
A Novel Approach for Treating Arthrogenic Muscle Inhibition in Post-ACLR Patients?
Hart JM, Kuenze CM, Diduch DR and Ingersoll CD.J Athl Training. 49:6, 740-746.
How many of you have
had the struggle of dealing with an ACLR patient that has suffered from an
inability to regain full volitional control of their quadriceps group? This is
a known pathology called Arthrogenic Muscle Inhibition (AMI) which has been
defined in the literature as an inhibitory reflex in response to damage that
has been suffered by the joint structures of the knee and it affects the
musculature surrounding the knee. It is currently theorized in this condition
that efferent input to the quadriceps has been inhibited in response to
“aberrant” afferent input from the joint and the amount of motor units
available for volitional control has been decreased.
Initially,
AMI may work as a protective reflex loop to protect the joint structures from
further damage. However, in the scenario of an athlete that has undergone
arthroscopic surgery to reconstruct an ACL injury it can be a burden that
prevents a return to pre-injury levels of strength and side-to-side
asymmetries. This condition would definitely be considered a detriment when it
prevents our patients from receiving the entire benefits from their
rehabilitation program and may wreak havoc upon their gait and other movement
patterns.
 |
| Source: http://www.physio-pro.com/files/2014/02/icing-the-knee1.jpg |
What if this could be
overcome with a simple and cost-effective intervention; perhaps an intervention
as simple and globally available as applying an ice-bag prior to exercise
intervention? Well that is exactly what this group of researchers did in this
current study. Hart et al built upon previous research that showed that Hoffman
reflex (h-reflex) could be increased when cryotherapy was used on subject’s
with inhibited quadriceps due to knee-joints that had been artificially
effused.
There is lot to discuss
when it comes to the intricacies of methods and procedures for this study and
the SMR already had a great post recently going over those details. You can
read their take in more
depth right here. On a global and applicable scale you
may be wondering what they found out. Well let me cut to the chase; using a
cryotherapy intervention immediately before performing rehabilitation exercises
resulted in better quadriceps function and strength gains compared to the other
interventions. This study was another brick laid for this theoretical
foundation and it is forming quite nicely. However, there is still more
research to do on this topic such as investigating other knee injuries like
PFPS, patellar tendinopathy, meniscal injuries, and longer intervention trials
>2 weeks are definitely warranted.
This study should be
kept in mind that sometimes cryotherapy is warranted. Especially at a time when
so many love to blindly point fingers at “passive modalities” such as cryotherapy.
Anything can be the perfect intervention if applied in the right place, at the
right time, and especially if it is guided by the right evidence. This is
something to keep in mind the next time you find yourself struggling with a
patient/athlete who is struggling to regain quadriceps function. It can’t hurt
to try (unless they have a cold allergy), uses something that is most likely
already located in your athletic training clinic, and has some promising
research in the works.





.gif)
.JPG)


